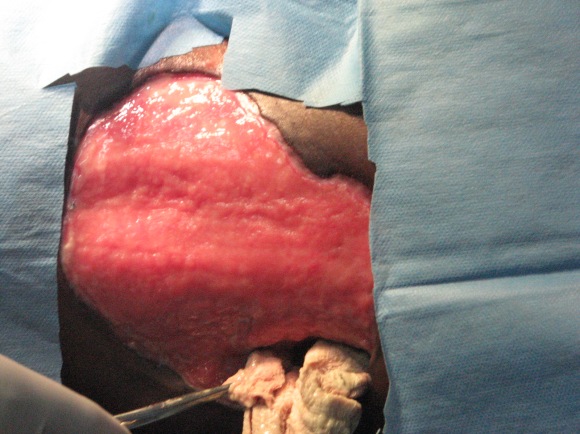
I have seen a ‘spontaneous’ colostomy in a strangulated hernia which presented after days of pain. But even more unusual, shortly after that I had 3 cases of lumbar colostomies in children. One was in a boy who fell onto a sharp stick which went into his right lumbar area. Faeces began to discharge immediately but he lived hours away in an area without roads and his parents were very poor. He lived and after 3 months they had enough money to travel to our hospital. By that time he had developed a huge ulcer as seen in the photo below.
The other two had a high fever and then burst pus and faeces from their right lumbar areas. They came soon after that and did not have the surrounding skin necrosis of the first boy. Neither this boy nor the other two had significant abdominal findings.



After some blood tests and an IV line inserted and being started on IV antibiotics, they all had a laparotomy. In each of them the posterior wall of the ascending colon was perforated and opened into a retroperitoneal abscess. They all had a limited right colectomy and primary closure of the intestine. The traumatic case was a little older and he had sufficient omentum to lay across the abdominal wall opening but the other two had their initial wounds repeatedly packed with saline soaked packs to stop the small intestine falling out the wounds. I thought that in the latter two cases the hole would have been related to a retro-colic appendix but in all three the hole was half way up the ascending colon. We saw many cases of perforated typhoid ulcers but they are in the small intestine.
When the bowels were working well and the wounds were clean the process of skin grafting the first boy and closing the defects in all three were carried out. I chose to raise a flap of anterior abdominal wall including the external oblique abdominal muscle.


The flaps worked well even if there was fairly major scar.


Here is one of the children seen from behind. Thin but recovering. The Caucasian doctor seen in the background was a visiting surgeon from Sweden. Many of the children had no clothes, nakedness didn’t concern anyone.
Barry Hicks

2 replies on “3 paediatric spontaneous lumbar colostomies”
Having had the privilege of working with Barry Hicks both as an OR nurse & his private practice nurse in the early 1990’s, I thoroughly enjoyed reading his articles & seeing the skills that I had seen with my own eyes in years past. Well done, Dr Hicks – God gifted you well !
LikeLike
Thank you Angie for your lovely comment. I loved surgery and thank God for calling me into that healing ministry. God bless!
LikeLike